Aqueduct Stenosis
Summary
- Narrowing of the Sylvian aqueduct can cause impaired CSF outflow resulting in either acute or chronic hydrocephalus
- Can be caused by a congenital web but may also be caused by midbrain tumours, haemorrhage or infection
Cases
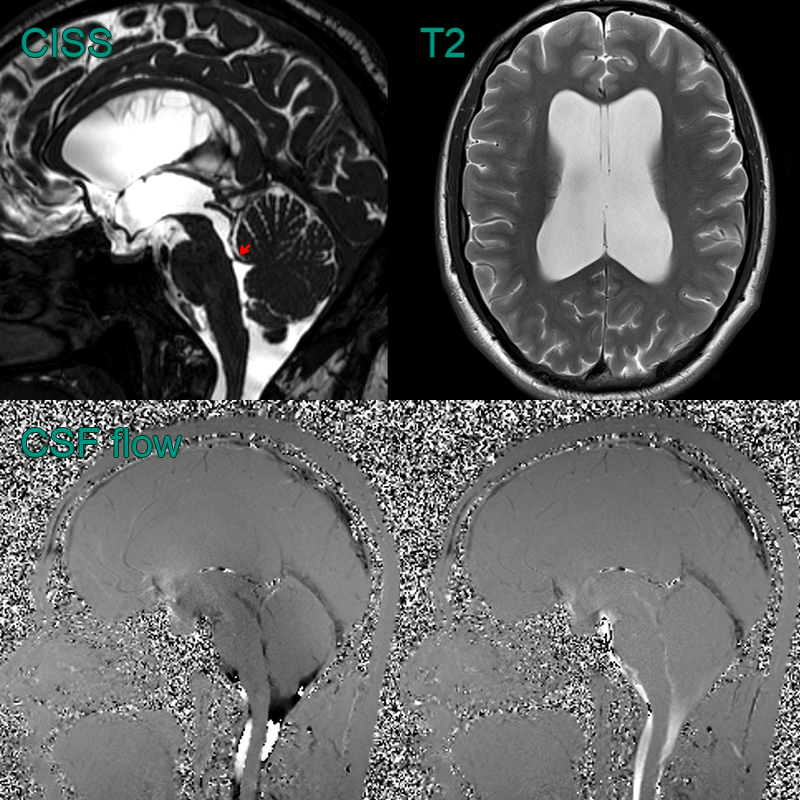
- A 40-year-old patient had an MRI scan due to chronic but increasing headaches
- MRI showed a focal filling defect in the inferior sylvian aqueduct
- CSF flow studies showed normal biphasic flow indicating a stenosis rather than an obstruction
Pathophysiology
- Narrowing or obstruction of the cerebral Sylvian aqueduct resulting causing impaired CSF drainage and increase intraventricular pressure
- Typically a longstanding lesion, hydrocephalus is usually compensated (i.e., no periventricular oedema or sulcal effacement)
Demographics
- Most common cause of congenital hydrocephalus
- Incidence: 0.5-1 per 1000 live births
- Male predominance (2:1 ratio)
Diagnosis
- Clinical presentation (headaches, vomiting) and clinical findings (papilloedema, bulging fontanelle in infancy) usually relate to raised intracranial pressure
Imaging
- Dilated lateral and third ventricles
- Normal or small fourth ventricle
- Possible periventricular hypoattenuation (CT) or hyperintensity (T2-weighted imaging) due to oedema
- High resolution T2-weighted imaging (e.g., CISS or FIESTA) usually indicated to identify small aqueduct web
- CSF flow studies (midline sagittal and axial at level of Sylvian aqueduct) can be considered to qualitatively or quantitatively assess CSF flow across stenosis
Treatment
- Surgery considered when symptomatic or increasing ventriculomegaly:
- Endoscopic third ventriculostomy (ETV): preferred first-line treatment
- Ventriculoperitoneal (VP) shunt: alternative if ETV fails or is contraindicated
Differential diagnosis
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Communicating Hydrocephalus | All ventricles enlarged, including 4th ventricle |
| Normal Pressure Hydrocephalus | Typically affects older adults; triad of gait disturbance, urinary incontinence, and dementia |