Cerebral Amyloid Angiopathy (CAA)
- 75-year-old patient presented with abnormal sensation in the left arm.
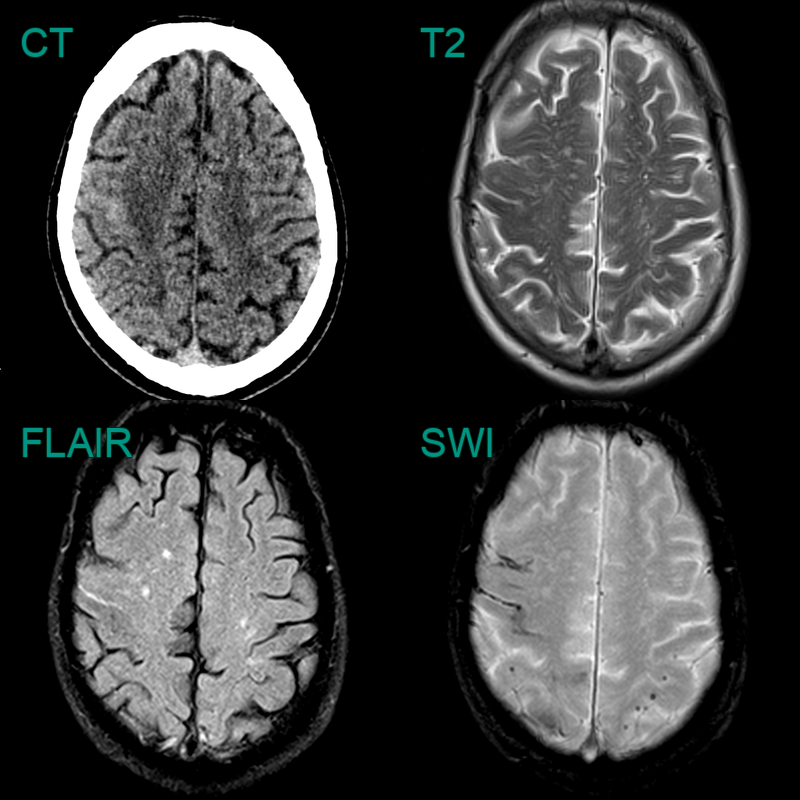
- CT showed blood product in the right pre-central gyrus.
- On MRI, there was sulcal hyperintensity on FLAIR consistent with recent blood product.
- Enlarged perivascular spaces, mutli-spot small vessel disease, superficial siderosis and lobar microhaemorrhages indicated a diagnosis of TFNEs secondary to CAA.
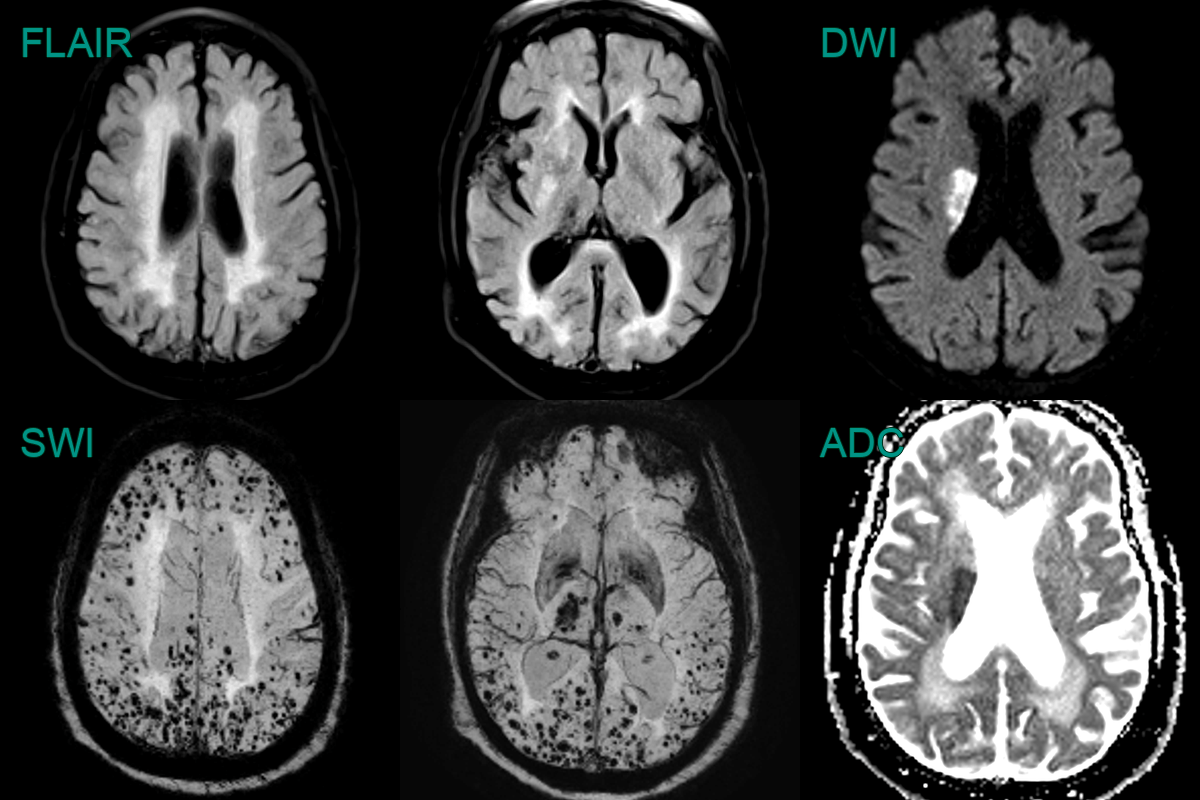
- Mulit-spot small vessel disease predominantly in the centrum semiovale, enlarged perivascular spaces and innumerable peripheral microhaemorrhages.
- Multi-spot small vessel disease, enlarged perivascular spaces, lobar microhaemorrhages, and extensive superficial siderosis indicate cerebral amyloid angiopathy.
- There was sulcal FLAIR hyperintensity in the right superior frontal sulcus and the left calcarine sulcus (not shown) that were associated with the left sided motor and right visual field TFNEs.
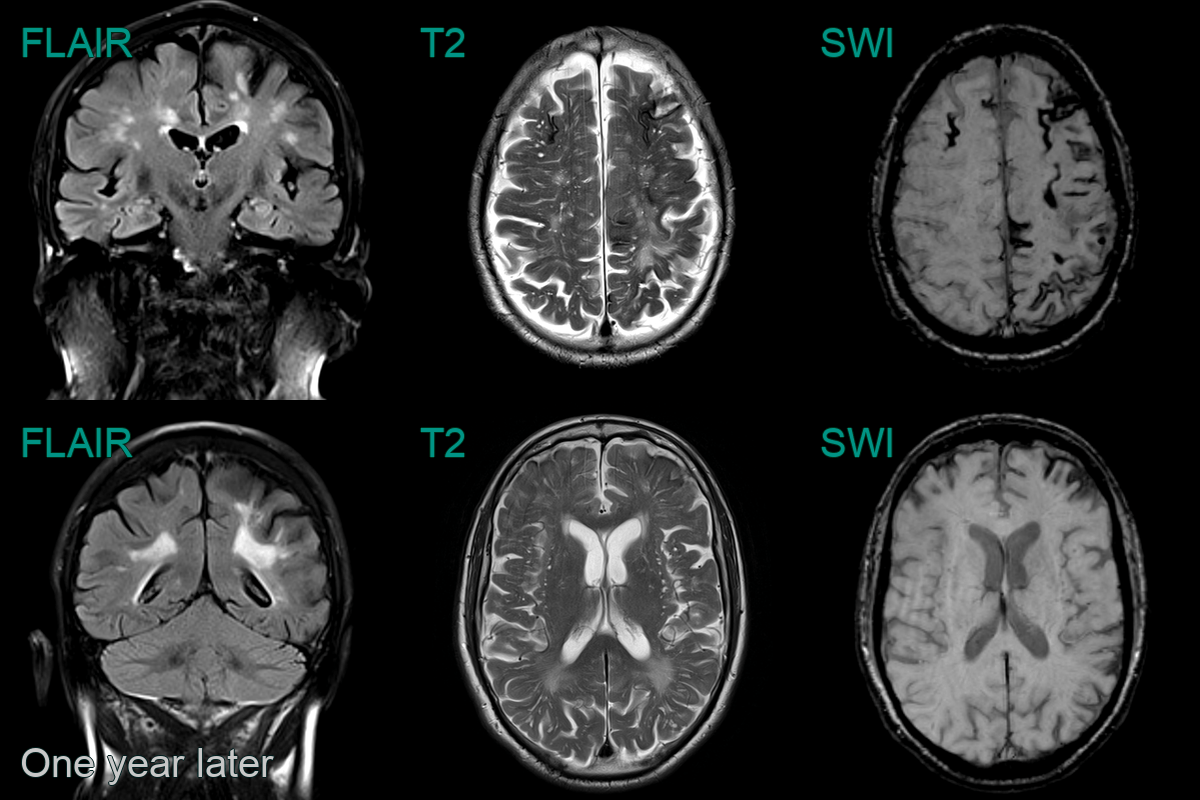
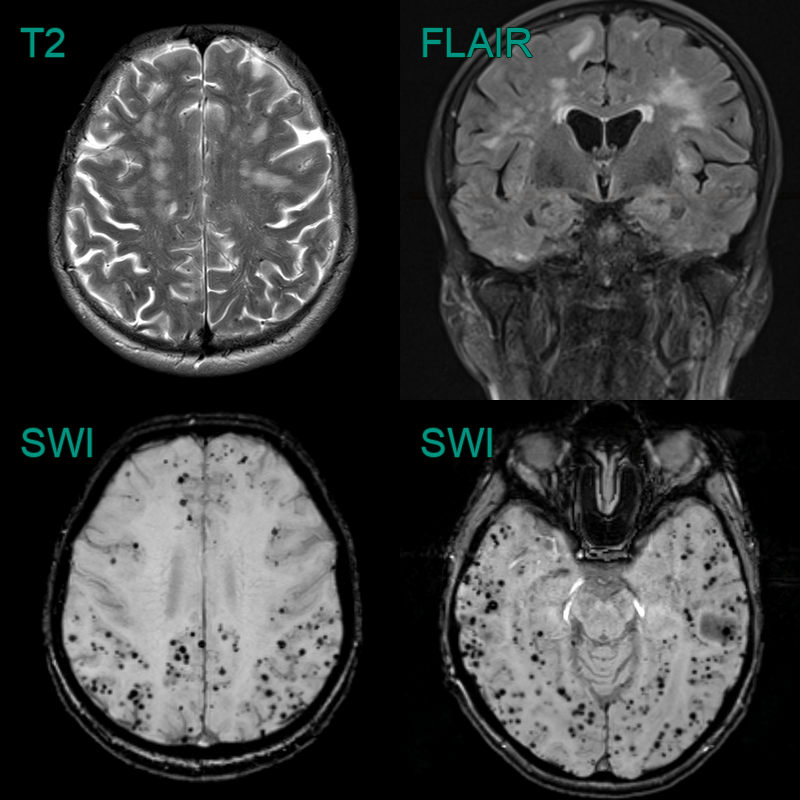
- 75-year-old patient presented with affecting right arm weakness.
- The initial MRI showed a lobar haemorrhage affecting the left precentral gyrus. There was a multi-plot pattern of (posterior-predominant) small vessel disease, many enlarged subcortical perivasular spaces, and extensive superfial siderosis but only a few few lobar microhaemorrhages.
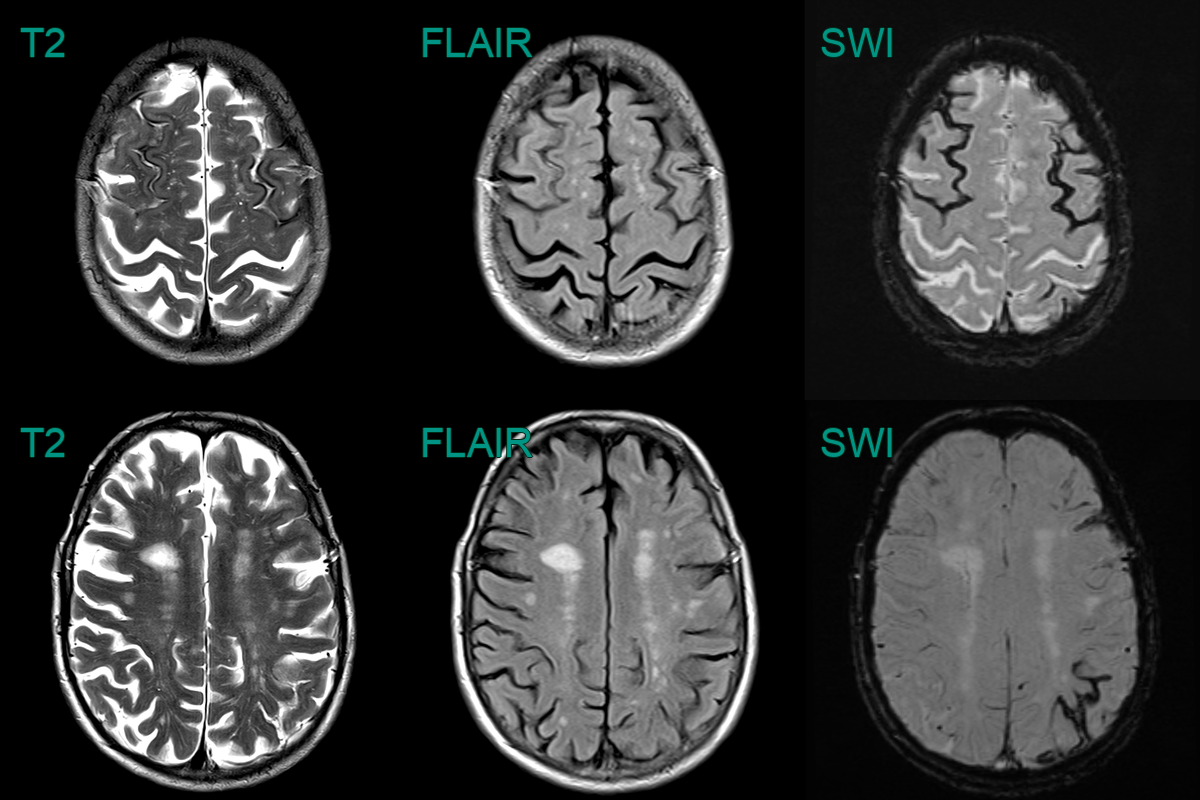
- A 75-year-old patient presented with left sided weakness.
- MRI showed an acute infarct in the right corona radiata.
- SWI showed florid microhaemorrhages in a mixed distribution - both deep (likely representing hypertensive arteriolosclerosis) and lobar (likely representing cerebral amyloid angiopathy).
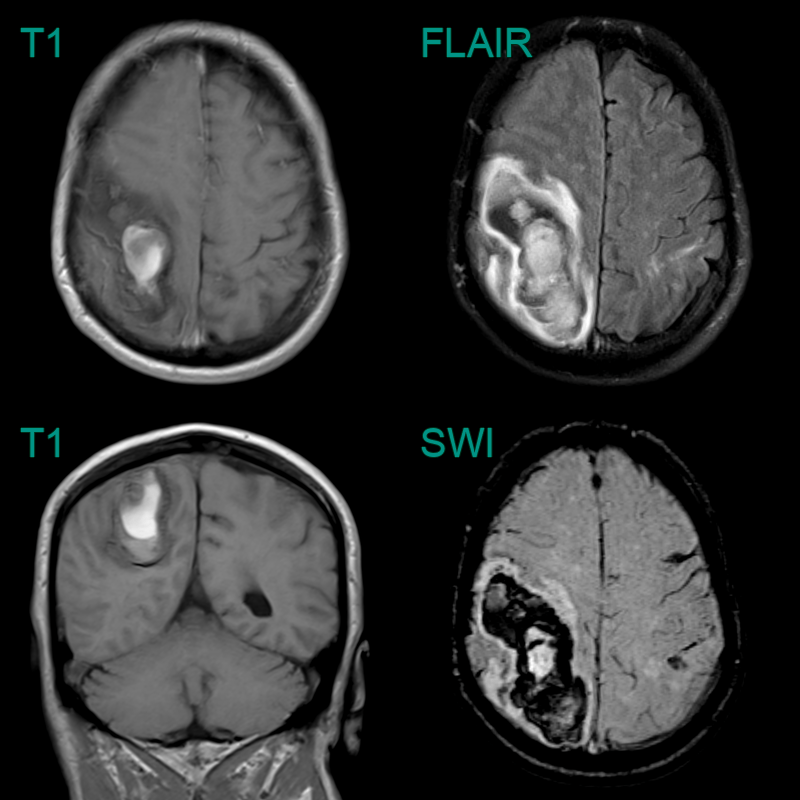
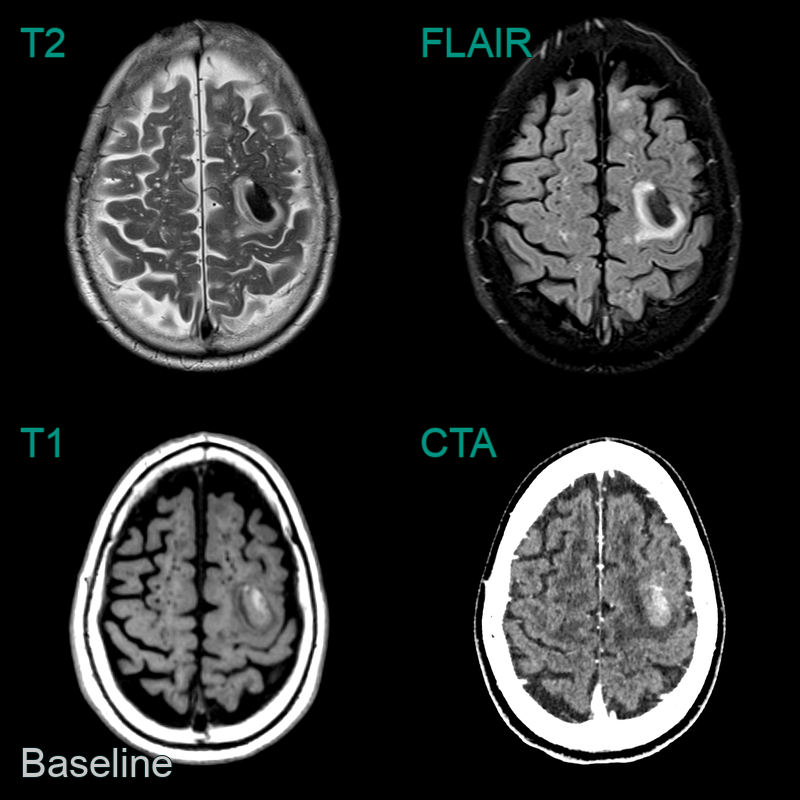
- A 65-year-old patient presented with headache and left sided weakness.
- MRI showed a large lobar haematoma in the right parietal lobe.
- There was a trace of acute blood in the left post-central gyrus (based on FLAIR hyperintensity).
- While there were no white matter features of CAA, the combination of the superficial siderosis over the left frontal lobe and the lobar haematoma were sufficent to meet criteria for probable CAA.

- A 70-year-old patient presented with transient senory distrubance in the left arm and left side of the face.
- MRI showed subarachnoid blood/effusion in the right central sulcus (red arrows) as a cause of the TFNE.
- SWI showed cortical microhaemorrhages (green arrows) and many areas of superficial siderosis.