Glioblastoma
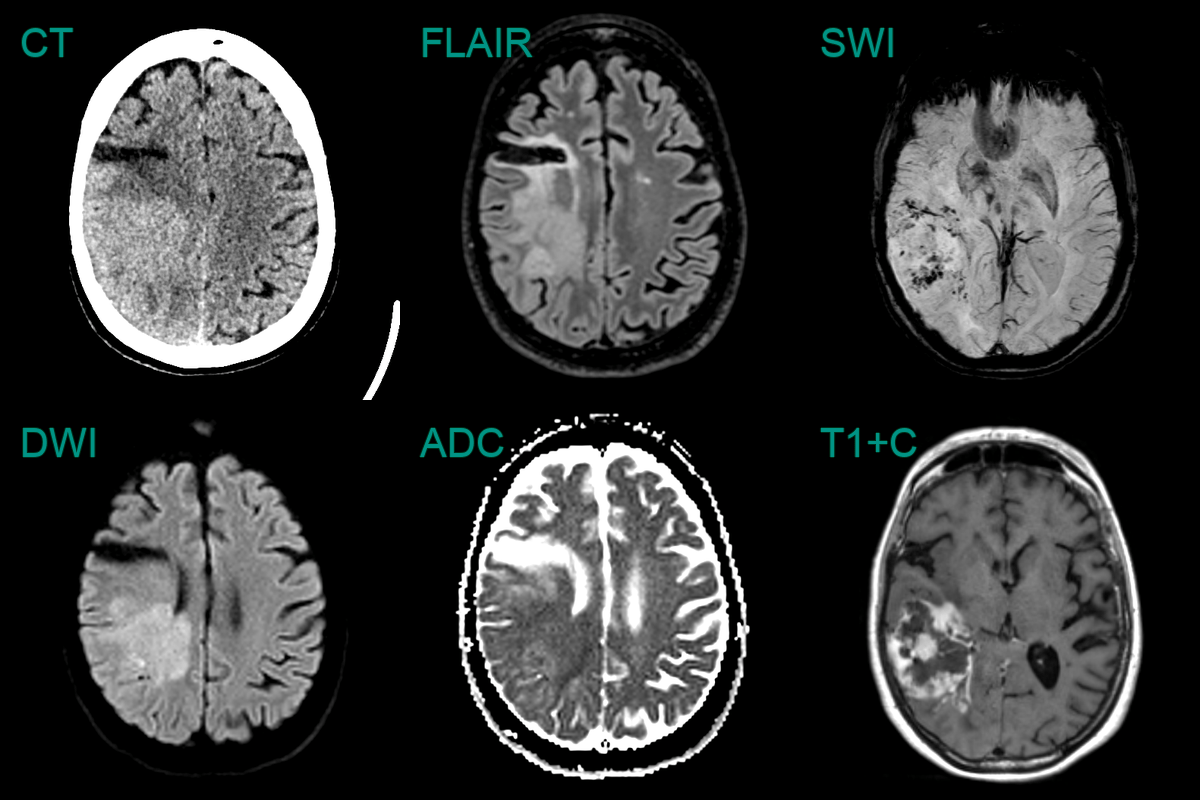
- 60-year-old patient, with a previous right MCA territory ischaemic stroke, presented with a left-sided homonymous hemianopia.
- CT showed a hyperdense mass lesion posterior to the old infarct.
- MRI showed a diffusion-restricting, peripherally enhancing mass lesion. SWI showed neovascularisation and microhaemorrhages within the lesion.
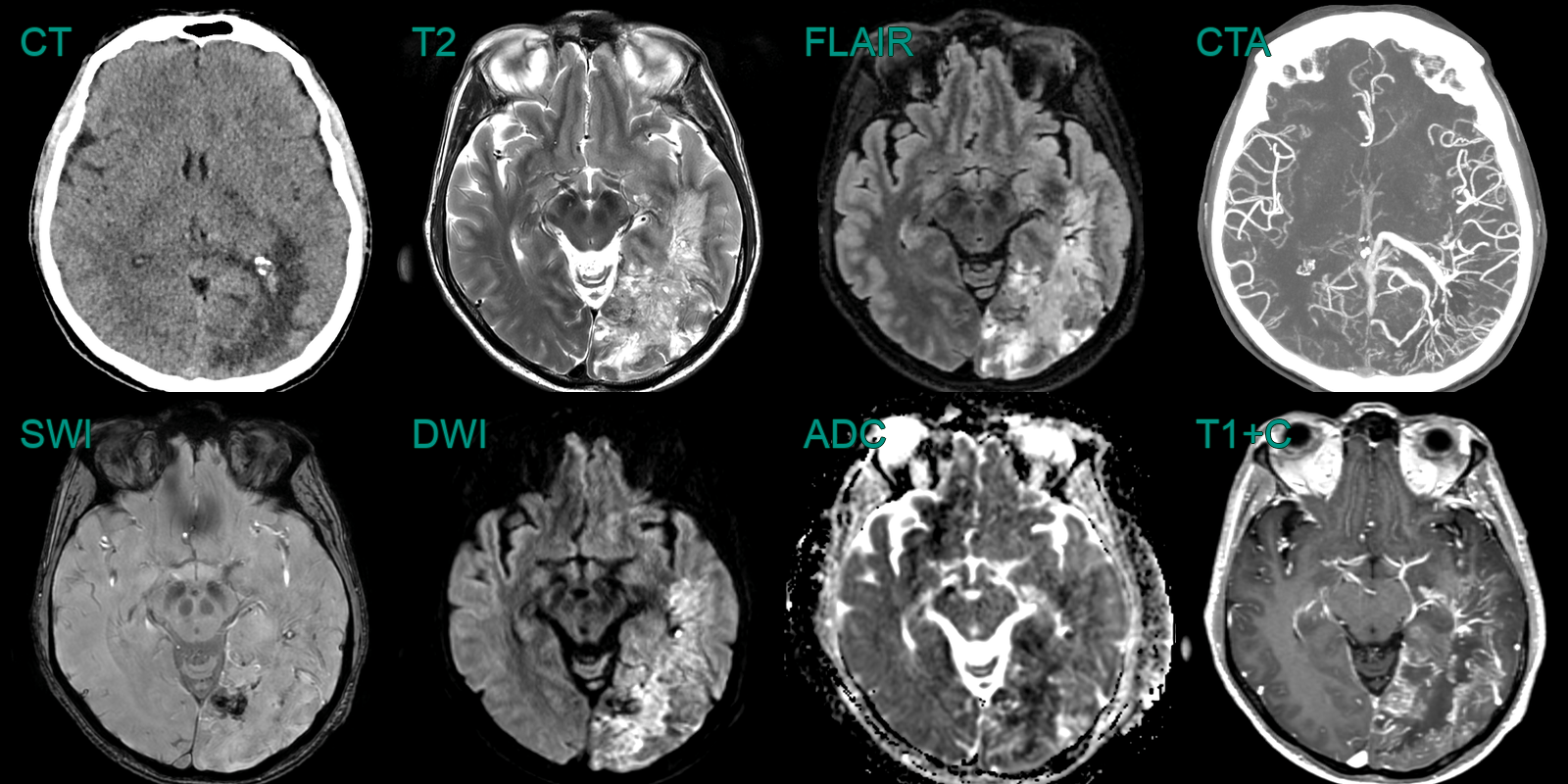
- A patient presented with a headache and on examination had a large right visual field defect.
- CT showed a larger left occipital lesion with striking (neo)vascularity.
- MRI showed a peripherally enhancing lesion causing diffusion restriction and containing small regions of blood product.
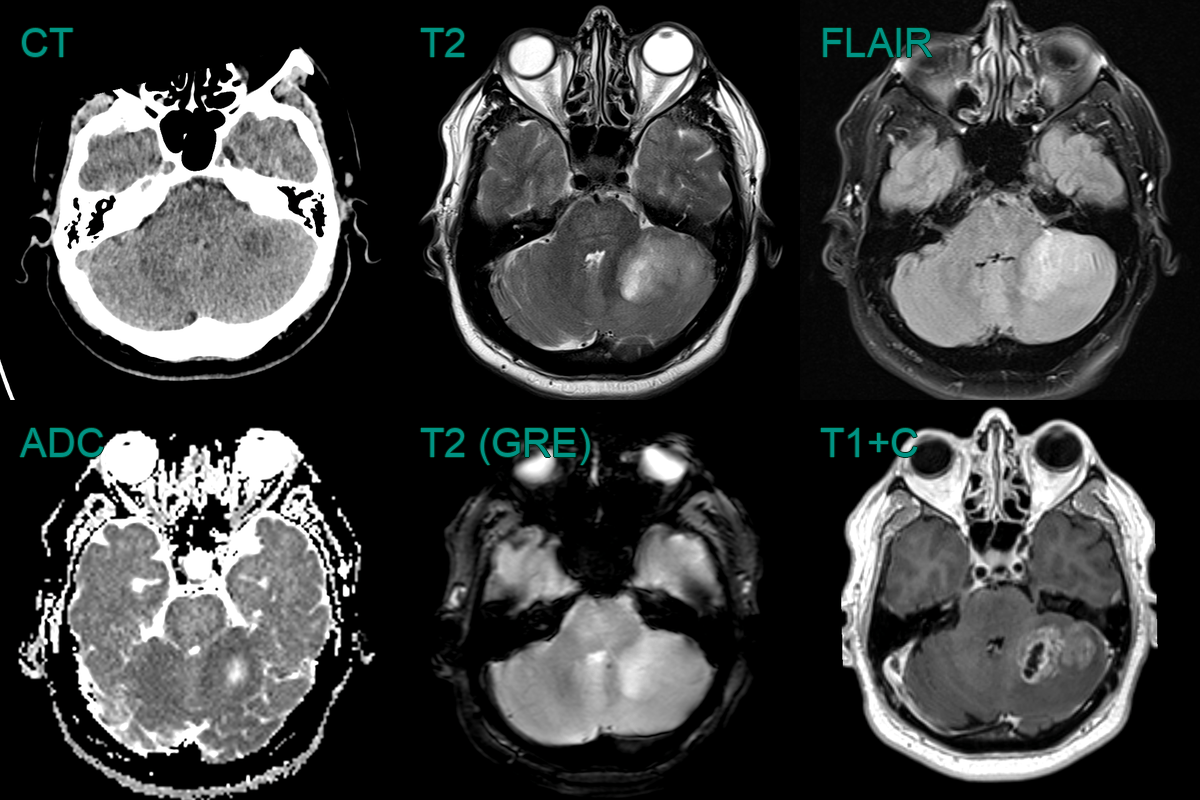
- 65-year-old patient presented with headache, nausea, vomiting and speech disturbance.
- Imaging showed a peripherally enhancing, centrally necrotic, left cerebellar mass lesion.
- ADC values were lower in the periphery of the tumour indiciating hypercellularity.
- Unusually for the cerebellum, histopathology revealed a glioblastoma.
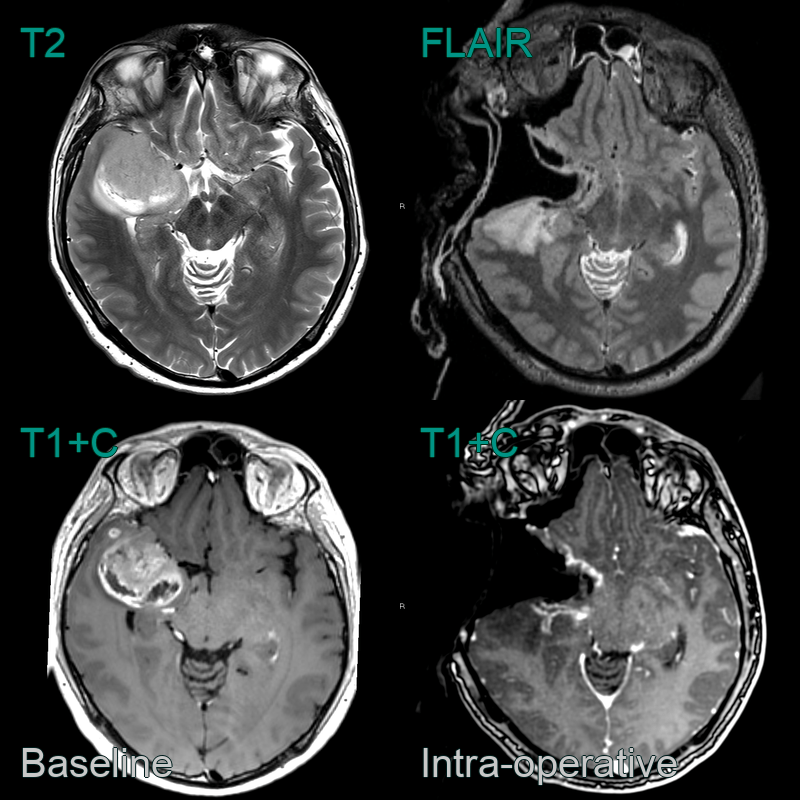
- A 50-year-old patient presented following a seizure.
- MRI showed a large right temporal peripherally enhancing lesion with areas of diffusion restriction (not shown).
- Intra-operative MRI was used to guide a maximal safe resection.
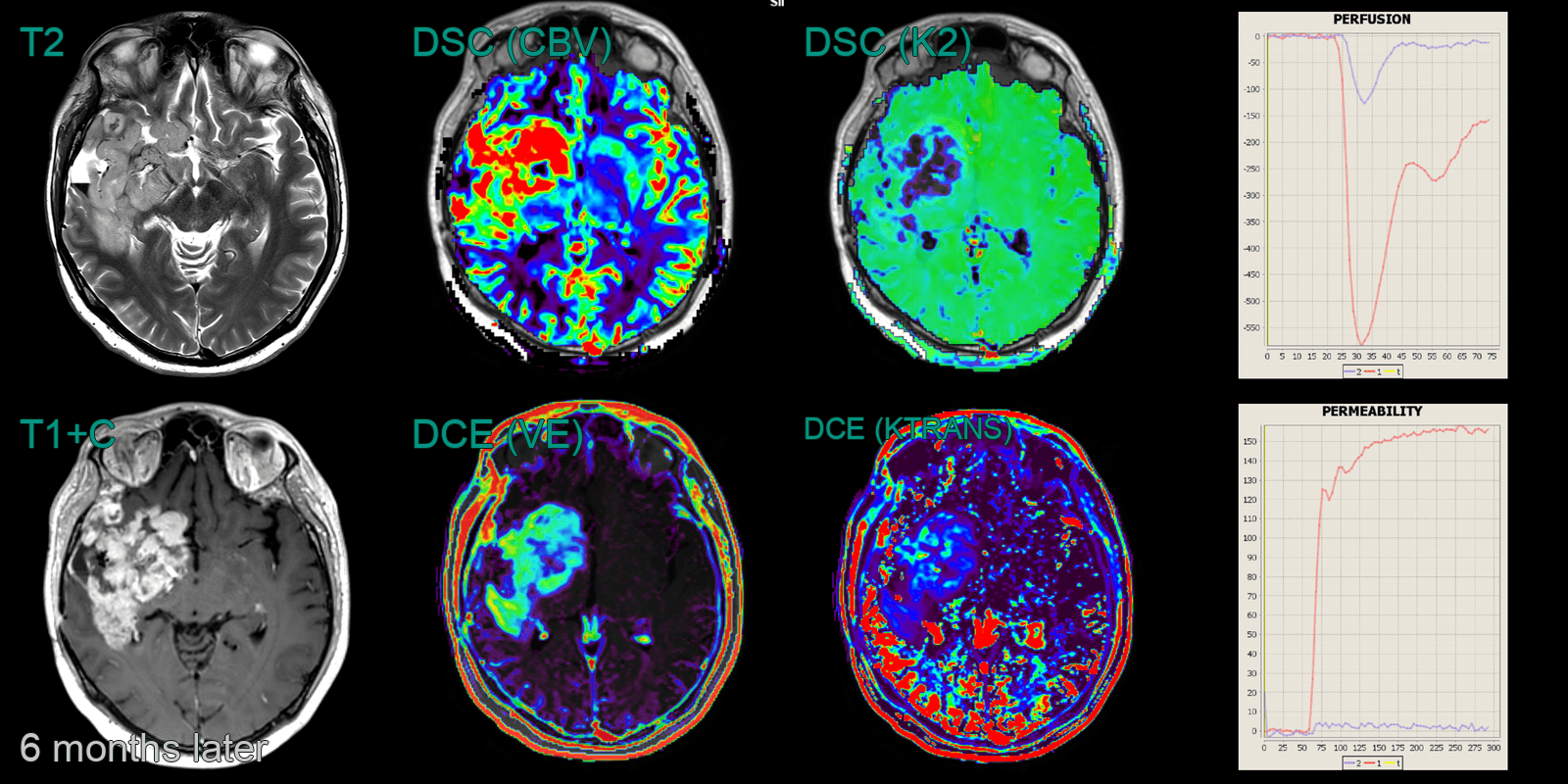
- Within 6 months, there was a large volume of disease progression. While obvious on structural imaging, this was confirmed on DSC perfusion (elevated CBV and abnormal K2) and DCE perfusion (elevated Ktrans and VE and a Type 2 curve).